

Abstract
Background This research explores how the COVID-19 pandemic has changed the ways doctors make end-of-life decisions, particularly around Do Not Attempt Cardio-Pulmonary Resuscitation (DNACPR), treatment escalation and doctors’ views on the legalisation of euthanasia and physician-assisted suicide.
Methods The research was conducted between May and August 2021, during which COVID-19 hospital cases were relatively low and pressures on NHS resources were near normal levels. Data were collected via online survey sent to doctors of all levels and specialties, who have worked in the NHS during the pandemic.
Results 231 participants completed the survey. The research found that over half of participants reported making more patients DNACPR than prepandemic, and this was due, at least in part, to an increased focus on factors including patient age, Clinical Frailty Scores and resource limitations. In addition, a sizeable minority of participants reported that they now had a higher threshold for escalating patients to ITU and a lower threshold for palliating patients, with many attributing these changes to formative experiences gained during the pandemic. Finally, our study found that there has not been a statistically significant change in the views of clinicians on the legalisation of euthanasia or physician-assisted suicide since the start of the pandemic.
Conclusion The COVID-19 pandemic appears to have altered several aspects of end-of-life decision making, and many of these changes have remained even as COVID-19 hospital cases have declined.
Data availability statement
Data are available on reasonable request.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
Background
The COVID-19 pandemic has transformed many aspects of clinical medicine, including, and perhaps especially, end-of-life care. This research aims to ascertain whether the pandemic, which has seen thousands more patients than normal require end-of-life care, has made a significant change to the ways doctors make end-of-life decisions.
There are three areas that this research focusses on:
-
‘Do Not Attempt Cardio-Pulmonary Resuscitation’ (DNACPR) Decisions.
-
Treatment escalation.
-
Views on euthanasia and physician-assisted suicide.
DNACPR decisions
At the start of the UK COVID-19 epidemic, there was an increased urgency among both hospital and community clinicians to make DNACPR decisions for their patients, in part due to the increase in cardiac arrests linked to COVID-19 infections.1 The Resuscitation Council UK issued a statement in March 2020 encouraging the early identification of patients for whom a DNACPR decision would be appropriate.2
However, a year into the pandemic, the Care Quality Commission (CQC) published a report which highlighted several areas of concern about DNACPR decision making during the pandemic.3 It found that 30% of patients surveyed with DNACPRs were not aware that a DNACPR had been put in place, and 35% felt they were not given sufficient information.3 The report also criticised the use of ‘blanket’ DNACPRs across over a hundred adult social care settings.3
In light of these developments and controversies, this research investigates if there has been a significant effect of the pandemic on DNACPR decision making in the National Health Service (NHS).
Treatment escalation
In March 2020, in response to concerns about Intensive Therapy Unit (ITU) capacity during the pandemic, The National Institute for Health and Care Excellence (NICE) published their ‘COVID-19 Rapid Guideline’, which stated that admission to ITU should only be considered if a patient is likely to recover and there is a clear plan for how organ support will lead to agreed treatment goals.4 It also recommended the use of Clinical Frailty Scores (CFSs) to guide treatment escalation decisions.4 These guidelines and considerations appear to have led to an increased focus on treatment escalation planning for COVID-19 patients; one observational study found that the majority (84.5%) of COVID-19 patients studied had documented ceilings of care.5
There has also been an increased focus on early palliative care intervention. Early in the pandemic, several journals including The British Medical Journal and The Lancet published articles guiding clinicians on early palliative care for patients with severe COVID-19 infection.6 7
This research aims to investigate if the pandemic has caused clinicians to raise their thresholds for referring or accepting patients to ITU, and/or lower their thresholds for palliation.
Euthanasia and physician-assisted suicide
In 2019 and 2020, the British Medical Association (BMA), Royal College of Physicians (RCP) and Royal College of General Practitioners (RCGP) polled their members’ views on the legalisation of physical-assisted dying. The RCP and RCGP surveys found the largest vote shares were opposed to the legalisation of physician-assisted dying.8 9 The BMA found their largest vote share was in favour of the legalisation of physician-assisted suicide but opposed to euthanasia.10
Significantly, all three surveys were carried out before the start of the pandemic. There is little data available on how the experiences of the pandemic have changed clinicians’ views on the legalisation of physician-assisted dying, if at all. This is of clear contemporary relevance in light of Baroness Meacher’s Assisted Dying Bill which is currently in the parliamentary committee stage.11
This research aims to find out if and how the pandemic has changed doctors’ views on the legalisation of euthanasia and physician-assisted suicide.
Methods
The research was carried out through online survey, distributed via NHS email, direct messengers and trusted social media outlets. The participation criteria was: all doctors from all specialties and all grades who have worked in the NHS at some point during the pandemic.
The survey consisted of a mixture of tick-box and free-text answers. The full survey can be found in online supplemental appendix 1.
Supplemental material
Following a pilot study conducted between April and May 2021, the survey was then distributed to participants between 6 May 2021 and 14 August 2021. During this time, national COVID-19 inpatient cases were relatively low, ranging from around 880 COVID-19 inpatients at its lowest to around 5900 at its peak.12 This is in comparison to the approximately 38 000 inpatient cases at the height of the second wave in January 2021.12
Results
Participants
The total number of participants who completed the survey was N=231, with no participants excluded from the data set. The participants were composed of 15 foundation year 1 doctors (6.5%), 146 senior house officers (SHOs) or equivalent (63.2%), 42 specialty registrars (SpRs) or equivalent (18.2%), 24 consultants or GPs (10.4%) and 4 others (1.7%).
Participants came from the whole range of clinical specialities, with the biggest representation coming from Internal Medicine and Accident and Emergency (A&E). 42.4% of respondents stated that they spent the majority of the pandemic working in Internal Medicine, and 20.8% in A&E.
DNACPR decisions
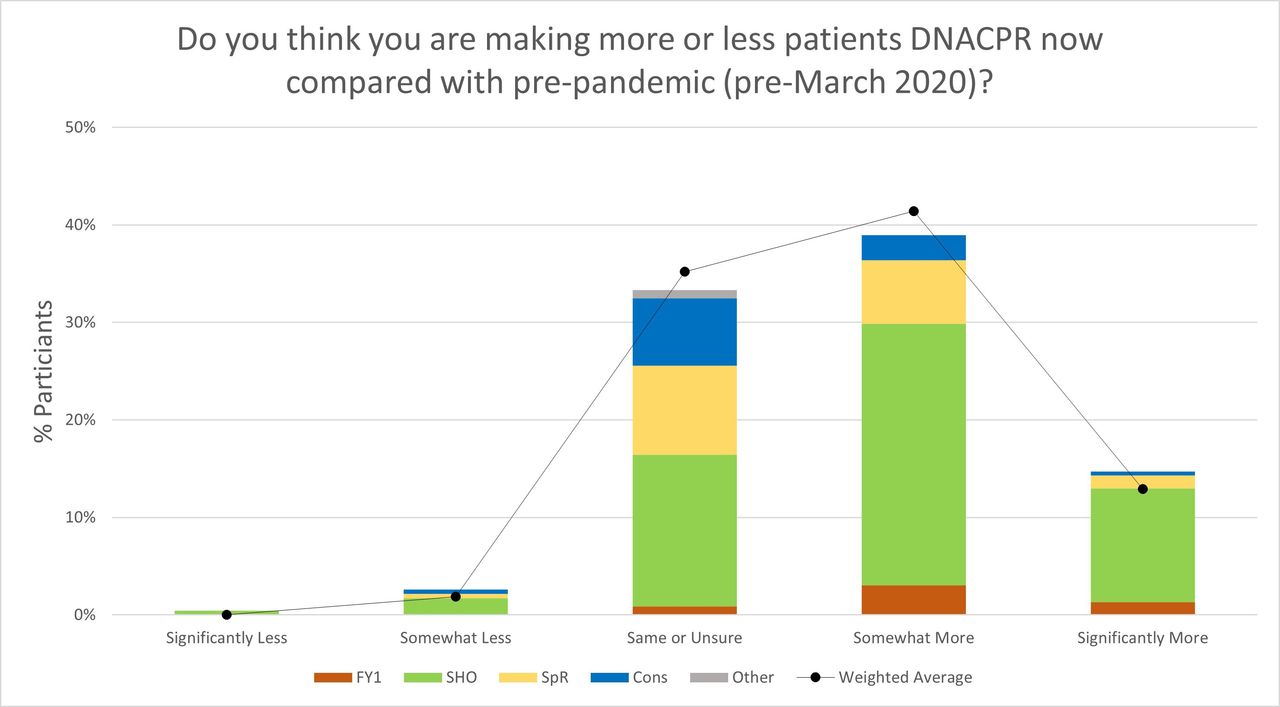
Participants were then asked if they were making more or less patients DNACPR now compared with prepandemic. As shown in figure 1, 0.4% of participants stated that they were making ‘significantly less’ patients DNACPR, 2.6% said ‘somewhat less’, 33.3% said ‘same or unsure’, 39.0% said ‘somewhat more’ and 14.7% said ‘significantly more’. 10.0% said the question was not applicable to their clinical situation. Weighted averages were then calculated so that results were proportionately representative of the different medical grades in the NHS national workforce (as of June 2021).13 When weighted for medical grades, the results were: significantly less—0.0%, somewhat less—1.9%, same or unsure—35.2%, somewhat more 41.4%, significantly more—12.9% and not applicable—8.6%.

Participants’ responses to the question ‘Do you think you are making more or less patients DNACPR now compared with pre-pandemic (pre-March 2020)?’. DNACPR, Do Not Attempt Cardio-Pulmonary Resuscitation.
In sum, over half of participants reported that they were making more patients DNACPR at time of data collection compared with prepandemic.
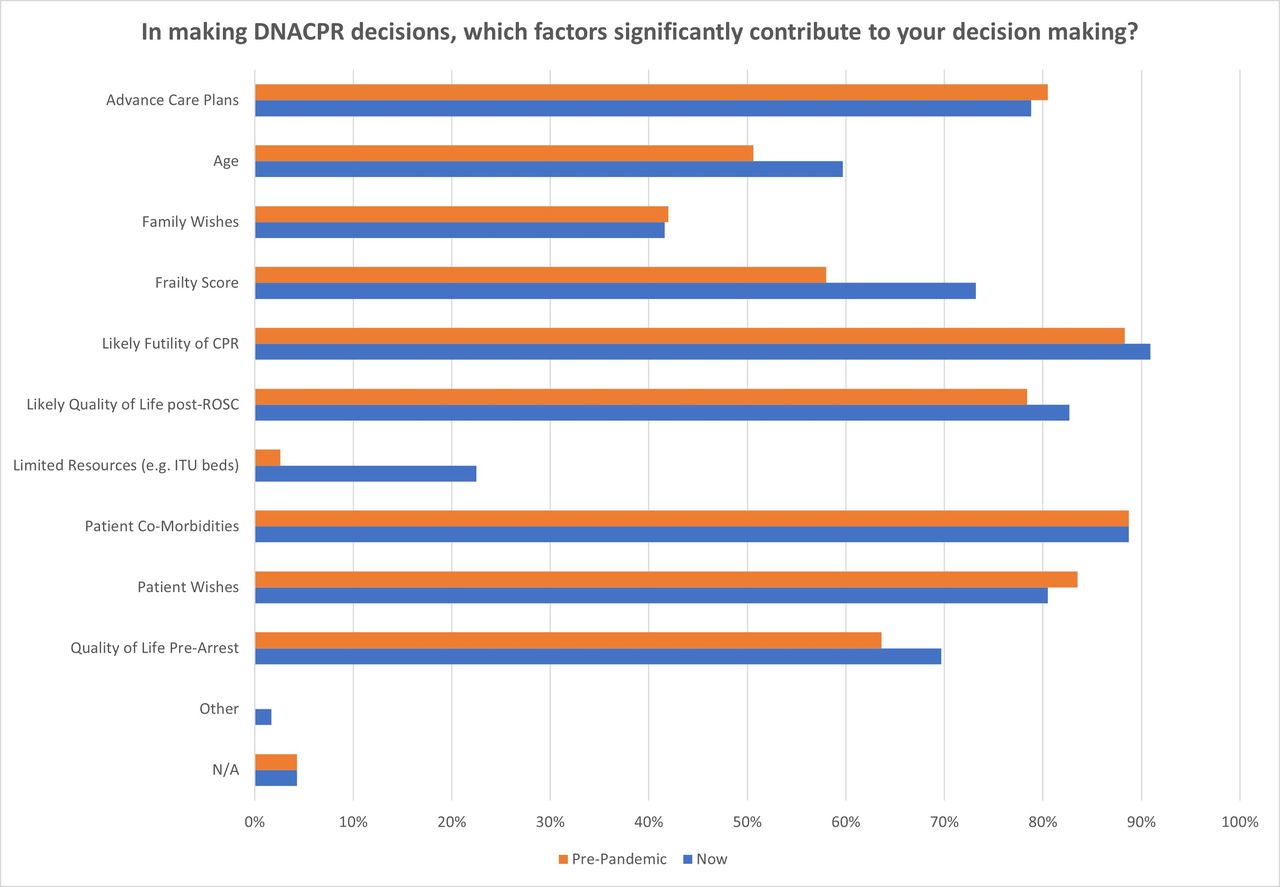
Participants were then asked to select which factors significantly contributed to their DNACPR decision making, both prepandemic and at time of the questionnaire (figure 2). The most cited factors were ‘likely futility of CPR’ (88.3% prepandemic, 90.9% now), patient comorbidities (88.7% both prepandemic and now), and patient wishes (83.5% prepandemic, 80.5% now). Advance care plans and ‘quality of life following return of spontaneous circulation (ROSC)’ also received large vote-shares.

Participants’ responses to the question ‘In making DNACPR decisions, which factors significantly contribute to your decision making?’. Orange bars pertain to practices prepandemic, blue bars pertain to practices at the time of questionnaire. DNACPR, Do Not Attempt Cardio-Pulmonary Resuscitation.
However, what is arguably more notable is the factors that saw the biggest change in vote share. There was a 9.1% increase in the number of participants who stated that ‘patient age’ was a significant contributing factor to DNACPR decisions, from 50.6% prepandemic to 59.7% at time of questionnaire. There was a 15.2% increase in those who selected CFSs, from 58.0% to 73.2%. But the biggest change in vote-share was for ‘resource limitation’ which saw a 19.9% increase, from 2.6% to 22.5%.
When participants were asked to explain in their own words why their decision-making processes may have changed, some common themes emerged including an increased sense of urgency among clinicians to make DNACPR decisions as early as possible in a patient’s admission, and a change in culture that encouraged clinicians to consider DNACPR decisions almost by default for all patients, rather than just those at high risk of cardiac arrest.
Treatment escalation
In the next section, participants were asked if they had a higher or lower threshold for referring (or accepting) patients to ITU compared with prepandemic, and whether they had a higher or lower threshold for palliating patients. As with the questions around DNACPRs, weighted averages were then calculated so as to be proportionately representative of the medical grades in the NHS workforce.
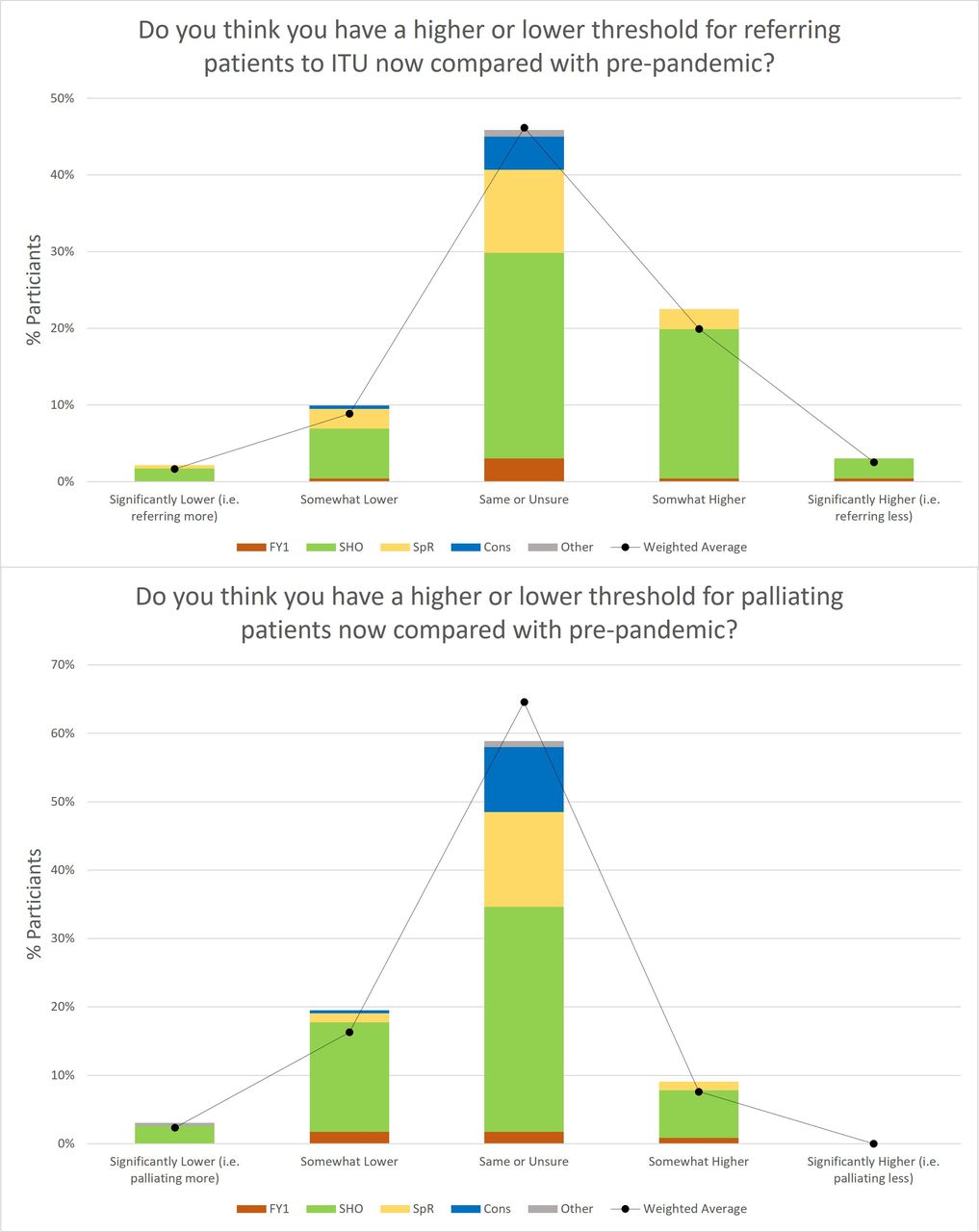
As shown in figure 3, when asked if they now had a higher or lower threshold for referring (or accepting) patients to ITU compared with prepandemic, 2.2% of participants reported that they had a significantly lower threshold (ie, referring more), 10.0% said somewhat lower, 45.9% said same or unsure, 22.5% said somewhat higher and 3.0% said significantly higher (ie, referring less). 16.5% reported that the question was not applicable to them. When results were weighted to reflect the portions of medical grades in the national workforce, the results were: 1.7% significantly lower, 8.9% somewhat lower, 46.2% same or unsure, 19.9% somewhat higher, 2.5% significantly higher and 20.8% not applicable.

Participants’ responses to the questions: ‘Do you think you have a lower or higher threshold for escalating patients to ITU, now compared with prepandemic?’ (top) and ‘Do you think you have a lower or higher threshold for palliating patients, now compared with prepandemic?’ (bottom). ITU, Intensive Therapy Unit.
When asked if they had a higher or lower threshold for palliating patients now compared with prepandemic, 3.0% of participants reported that they had a significantly lower threshold (ie, palliating more), 19.5% said somewhat lower, 58.9% said same or unsure, 9.1% said somewhat higher, and 0.0% said significantly higher (ie, palliating less), with 9.5% reporting that the question was not applicable to them. When results were weighted to reflect the portions of grades nationally, the results were: 2.4% significantly lower, 16.3% somewhat lower, 64.6% same or unsure, 7.6% somewhat higher, 0.0% significantly higher and 7.7% not applicable.
In sum, the largest vote share on both questions was for ‘same or unsure’—46.2% (weighted for grade) for escalation to ITU, and 64.6% for palliation. For the largest proportion of doctors, the pandemic has not significantly changed their treatment escalation thresholds. However, it is also notable that a substantial minority of respondents reported that they now have a higher threshold for referring to ITU (22.5% weighted) and lower threshold for palliation (18.6% weighted).
Participants were then asked to explain their potential changes in escalation thresholds. The most common theme in these responses was that working in the pandemic had given clinicians unique, intensive and formative experiences in managing critically unwell patients. For example, one respondent answered: ‘Seeing the amount of suffering on ICU has definitely made me reconsider whether many patients would tolerate or want it’, while another wrote: ‘COVID was vicious… Palliation meant allowing a comfortable death… I think we all realised there was no good in prolonging the suffering.’
Euthanasia and physician-assisted suicide
Participants were next asked for their views on the legalisation of euthanasia and physician-assisted suicide, both prepandemic and at time of questionnaire.
As shown in figure 4, 32.5% of respondents stated they were strongly opposed to the legalisation of euthanasia prepandemic, 14.7% were somewhat opposed, 20.3% were neutral or unsure, 21.2% were somewhat in favour and 11.3% were strongly in favour. When asked for their views on the legalisation of euthanasia now, there were some marginal changes. 32.9% of respondents stated they are now strongly opposed, 14.3% are somewhat opposed, 18.2% are neutral or unsure, 23.4% are somewhat in favour and 11.3% are strongly in favour. These results were analysed by 2×5 contingency tables (ie, χ2 analysis). Statistics were: χ2=0.55, 4 df, p=0.96.

When asked about their views on the legalisation of physician-assisted suicide pre-pandemic, the results were: 37.2% strongly opposed, 13.9% somewhat opposed, 24.2% neutral or unsure, 15.6% somewhat in favour and 9.1% strongly in favour. When asked about their views at present, there were marginal changes similar to the question about euthanasia. 36.8% of participants are now strongly opposed, 14.7% somewhat opposed, 22.5% neutral or unsure, 17.3% somewhat in favour and 8.7% strongly in favour. Statistics were: χ2=0.45, 4 df, p=0.97.
In sum, on both the questions about the legalisation of euthanasia and physician-assisted suicide, our results showed that the pandemic has led to marginal changes in views, which do not appear statistically significant (p>0.05) and are therefore probably due to chance.
Discussion
Participants
Our participants (N=231) were drawn from the spectrum of UK clinicians.
There was a high representation of junior doctors, particularly SHOs who made up 63.2% of respondents, compared with 17.5% of the national workforce.13 The main reason for this over-representation of junior doctors is likely because the survey was propagated mostly via Whatsapp and other social media channels, which are predominately populated by junior, rather than senior, doctors. This over-representation of junior doctors was partly addressed through the calculation of weighted averages for the responses to the questions around DNACPR and treatment escalation decisions, in order to better reflect the proportions of medical grades nationwide.
There was also a high representation of clinicians who worked in Internal Medicine and A&E during the pandemic. The obvious reason for this was that during the peaks of the pandemic, large numbers of medical staff were ‘redeployed’ away from elective and community services and into acute settings.14
One priority was to obtain a range of opinions on euthanasia and physicians-assisted suicide. When asked about their views on the legalisation of euthanasia prepandemic, the vote proportions were relatively similar to the results of the 2019 RCP survey (figure 5) and therefore deemed a satisfactorily representative range of ethical views.8

Comparison between the Royal College of Physicians’ (RCP) 2019 survey on assisted dying (left) and our participants’ responses to the question ‘How would you describe your views on the legalisation of euthanasia, prepandemic?’ (right).
DNACPR decisions
This research found that over half of participants reported that they were making more patients DNACPR than prepandemic (figure 1). This almost certainly reflects a large increase in the number of patients being made DNACPR. Unlike the CQC report into DNACPR decisions during the pandemic,3 these figures pertain to practices at a time when COVID-19 hospital rates were relatively low, rather than during the peaks of the epidemic. Our results show that the strong impetus to make more patients DNACPR, that was brought on by the pressures of the pandemic, remained among many clinicians even when COVID-19 hospital cases returned to relatively low levels.
When participants were asked to select factors that significantly contributed to their DNACPR decision making, both prepandemic and now, the factors that saw the biggest increase were: age, CFSs and resource limitation (figure 2). General Medical Council (GMC) guidelines state that DNACPR decisions should be based on the likelihood of successful CPR, and the weighing up of the risks/burdens and benefits of CPR.15 Thus, the key question is whether this increased focus on age, CFSs and resource limitation is still within the ethical limits of GMC guidance.15
One could argue that the increased focus on age and CFSs is compatible with making decisions based on the likelihood of successful CPR. For example, one meta-analysis found that CFSs were highly predictive for mortality.16 One could thus conclude that the pandemic has trained clinicians in how to efficiently make judgements around the likelihood of successful CPR, by the increased utilisation of factors such as age and CFSs. However conversely, others could argue that CFSs are a measure of social dependence rather than medical comorbidities,17 and so basing clinical decisions on CFSs is potentially discriminatory against the socially vulnerable.18
But what appears irreconcilable with GMC guidance15 is the increased focus on resource limitation, which saw the largest increase in vote share (from 2.6% to 22.5%). At the start of the pandemic, the BMA advised clinicians that in the event of NHS resources becoming unable to meet demand, resource allocation decisions should follow a utilitarian ethic.19 However, what is clear from our results is that for a significant proportion of clinicians, resource limitation continued to factor into clinical decision making even when pressures on NHS resources had returned to near-normal levels. This clearly falls outside the GMC guidance to base DNACPR decisions on the likelihood of successful CPR and weighing up the risks and benefits for each individual patient.15 Such findings indicate a subtle shift away from patient-centred DNACPR decision-making as mandated by the GMC,15 and towards a more utilitarian approach as suggested by the BMA at the start of the pandemic.18 19
Treatment escalation
The next part of this research focused on the effect of the pandemic on treatment escalation decisions. Despite the unique circumstances of the pandemic, the majority of participants reported that they had not changed their thresholds for escalation to ITU, or for palliation (figure 3).
However, nearly a quarter of respondents (22.5% weighted for grade), reported that they now had a higher threshold for referring patients to ITU than prepandemic, despite the data being collected when pressures on ITU resources were comparable to normal levels for the NHS. Participants’ comments showed that this increased threshold was largely due to a greater understanding of ITU care gained during the pandemic, including around its risks, burdens and limitations.
Furthermore, a sizeable minority (18.6% weighted) of respondents reported that they now had a lower threshold for palliating patients. When asked to explain, several participants noted that the pandemic had further educated them in the early recognition of dying patients, and the value of early palliative care.
Thus, the COVID-19 pandemic appears to have given some clinicians a formative education on the burdens and limitations of ITU care, and the value and appropriateness of early palliation. This has led to a sizeable minority of clinicians reporting an increased threshold for escalation to ITU, and decreased threshold for palliation.
Euthanasia and physician-assisted suicide
Finally, our research looked at clinicians’ views on the legalisation of euthanasia and physician-assisted suicide. The results showed that pre-pandemic, the largest proportion of participants were opposed to the legalisation of both euthanasia and physician-assisted suicide. When participants were then asked for their views at present, the vote proportions remained similar with only marginal changes. Using χ2 analysis, these changes were found to be statistically insignificant (p>0.05) and therefore likely due to chance.
Therefore, our results indicate that the pandemic has not, thus far, led to a significant shift in clinicians’ views on the legalisation of euthanasia or physician-assisted suicide.
Challenges and limitations of the research
There were several challenges and limitations that were encountered during this research.
First, the participant pool was limited to clinicians accessible via digital media outlets. This mode of data collection disproportionately selected for junior-level doctors who are more likely to regularly use these digital applications.13 In our study, this was partly addressed by calculating weighted averages for the responses to the questions around DNACPR and treatment escalation decisions. However, further research particularly among more senior clinicians would be valuable to add to our findings.
Second, we found that a large proportion of respondents spent the majority of the studied period working in Internal Medicine or A&E. This was due in part to the redeployment of NHS staff during the peaks of the epidemic. It is possible that this may have affected the results on DNACPR and treatment escalation decisions, as some staff may have been transferred from contexts where these decisions are not routinely made, to contexts in which they are. However, when participants were asked for the reasons why their decision making may have changed, no participants referenced this.
Third, there were some aspects of the survey that were not applicable to some clinicians. For example, some participants noted that they started clinical practice during the pandemic and therefore could not comment on their practice prepandemic, while some specialists noted that they do not routinely conduct some of the end-of-life decisions explored in the survey. We felt it important to still record these ‘not applicable’ responses in the summaries of the results.
Fourth, the survey focused on doctors’ perceptions of their decision making rather than on the decisions themselves. It is conceivable that some doctors may report changes in decision making processes that nonetheless do not manifest in significant objective differences in clinical decisions. It is also possible that some participants may not have accurately been able to recall their views or decisions prepandemic. It is of obvious relevance to patient care to study the effects of COVID-19 on objective clinical decisions. However, we suggest that it is also valuable to survey the attitudes and perceptions of clinicians in light of the pandemic, which have the potential to shape clinical practice well into the future.
Fifth, the vocabulary in the questionnaire had to be carefully chosen so as not to convey researcher bias, particularly on the controversial issue of assisted dying. However, in order to clearly delineate the issues being explored, the specific terms ‘euthanasia’ and ‘physician-assisted suicide’ were selected, rather than the vaguer term ‘assisted dying’, which the BMA defines as encompassing both euthanasia and physician-assisted suicide.10
Sixth and finally, the study was limited by the fact that data collection was carried out while the COVID-19 pandemic was still ongoing. The aim of the research was to look at whether COVID-19 has produced an ongoing change in the ways doctors make end-of-life decisions. To this end, data collection was carried out in Summer 2021 when COVID-19 hospital cases were relatively low. However, the peaks of the pandemic were still well within the recent memory of all participants, and COVID-19 cases were still fluctuating. It would therefore be valuable to repeat this research in a few months or years to investigate whether the changes in clinical practice that we have identified have become more permanent.
Conclusion
This paper has explored the differences COVID-19 has made to end-of-life decision making. Over half of clinicians surveyed reported that they are now making more patients DNACPR than prepandemic, and a sizeable minority reported that they now have a higher threshold for referring to ITU, and lower threshold for palliation. Views on euthanasia and physician-assisted suicide appear to have stayed the same.
What is yet to be determined is whether these changes will now stay the same indefinitely, revert back to prepandemic practices or evolve even further. Thus, this paper is only the beginning of the important exploration into how COVID-19 is changing the ways doctors make end-of-life decisions.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by St Mary’s University Twickenham, Ethics Sub-Committee Approved at Level 2 by Ethics Representative, Reference number: SMU_ETHICS_2021-22_225. Participants gave informed consent to participate in the study before taking part.


{kind=link}
{kind=link}
{kind=link}