

The Netherlands has just followed the UK and Ireland in opening up shops and restaurants and thus effectively ending its lockdown. As a visitor to the Netherlands, I was optimistic that the damning international data on vaccine efficacy against infection would have persuaded them to ditch their vaccine pass system immediately rather than dragging out the charade even longer. Alas, the Dutch government has decided to keep the vaccine passport system in place, disregarding the mountain of evidence that vaccine passes are now a sheer irrelevancy from an epidemiological perspective.
The Netherlands is not alone in embracing the naive hope that a vaccine passport scheme would somehow help them muddle through the last phase of the pandemic. This same hope was embraced until very recently in the UK and Ireland, and is still nourished, it would appear, by places where the vaccine pass schemes remain operative, such as Germany, Italy, France, Sweden, Canada, parts of Spain, and numerous US states.
The EU Commission trumpets its own vaccine certification scheme as “a success story of the EU. The Certificate continues to facilitate safe travel for citizens across the European Union during these times of the pandemic.” Yet both from an ethical and epidemiological perspective, the continuing reliance of free, post-Enlightenment societies on these discriminatory schemes is embarrassing and indefensible.
In what follows, I make the case that emerging evidence on vaccination effectiveness blows the case for vaccine passports out of the water, even on pragmatic, utilitarian grounds. But before we get into the utilitarian case against vaccine passports, it is important to point out that there are weighty ethical reasons for disqualifying a vaccine passport scheme – even in the best case scenario, in which it successfully curbs disease – as an entirely inappropriate tool of disease control in a society that values individual liberty and personalised healthcare.
The Ethics of Vax Passes
We have reason to oppose any public health scheme that effectively delegates citizens’ most intimate health choices to a remote body of “experts” who allegedly know what’s best for everyone. Any vaccine passport scheme of the sort that is now endorsed by leaders of the “free world” makes it impossible for patients and their doctors to exercise a reasonable margin of prudence and discretion in the management of health risks, since any deviation from the officially mandated course of action (in this case, “everyone must vaccinate”) must be justified to public officials by an extraordinary legal exemption, rather than freely decided by the patient in consultation with his or her doctor.
We should fiercely resist the temptation to treat human beings as disease vectors to be manipulated by algorithms, rather than as persons to be respected as ends in themselves. Erasing individual liberty is not an acceptable price to pay for the promotion of a public health goal. Nonetheless, since advocates of vaccine passports repeatedly insist that excluding the unvaccinated from public venues will yield great public health benefits, or make the world “safer” from Covid-19, let’s bracket our ethical misgivings for a moment, to consider the utilitarian case for vaccine passports on its own terms.
The Utility of Vax Passes: Are They likely to Reduce Disease Transmission?
There are two principal justifications for retaining a vaccine passport system either domestically or internationally:
(i) that they reduce community transmission of Covid-19, or
(ii) that they can incentivise people into making the best possible choices for their own health, yielding better health outcomes for the individual citizen, and alleviating the cumulative pressure on the health system.
The reason given by advocates of vaccine certificates, as we can see in the EU Commission’s own declarations about facilitating “safe travel,” is typically the first of the above, namely that they help us to combat disease transmission. So let’s consider this justification first. Are vaccine passes likely to reduce community transmission of Covid-19?
The short answer is, no, they are not. The balance of evidence overwhelmingly demonstrates that vaccine pass schemes, as efforts to reduce Covid transmission, are a fool’s errand. Since neither the Dutch public health authorities, nor the European Commission, nor the French government, nor the Italian government, nor the US Center for Disease Control, nor the US Food and Drug Administration, seem interested in publishing the relevant evidence, I’ve taken some time to compile some of it myself.
1. Evidence for Waning Vaccine Immunity
There is a strong international consensus at this stage that the immunity Covid vaccinations confer against infection diminishes progressively and substantially within a few months. According to the European Medicines Agency, “results from recently published studies show that vaccine effectiveness against symptomatic disease is lower for Omicron than for other variants and tends to wane over time” (emphasis added).1
One of Israel’s leading vaccine experts, Professor Cyrille Cohen, who heads the Laboratory of Tumor Immunology at Bar Ilan University and serves on Israel’s national advisory committee for clinical trials on SARS-COV2, recently observed in an interview with Freddie Sayers that with the advent of Omicron “both (vaccinated and unvaccinated persons) can get infected, more or less at the same pace.”
It is tempting to think that we could overcome the problem of waning vaccine immunity by just administering “boosters” on a regular basis. Assume, for example, that vaccines no longer protect against infection within, say, 4-5 months. Shouldn’t we just boost everyone every 4 months?
There are two reasons why this is a non-starter: first, logistically, it would be very complicated to roll out a population-wide vaccination campaign every 4 months indefinitely; second, and more importantly, this would be yet another population-wide medical experiment, which we cannot be confident is safe. The European Medicines Association has already warned that “too many doses of COVID-19 vaccines could eventually weaken the body’s immune system, rendering the extra shots ineffective,” as reported here.
The European Union’s drug regulator is warning that too many doses of COVID-19 vaccines could eventually weaken the body’s immune system, rendering the extra shots ineffective. Marco Cavaleri, the head of vaccine strategy for the European Medicines Agency, said earlier this week that booster shots can be administered “once, or maybe twice, but it’s not something that we think should be repeated constantly.” Cavaleri said instead that boosters should be administered just like an annual flu vaccination.
This advice was echoed by the World Health Organisation, as reported here.
A vaccination strategy based on repeated booster doses of the original vaccine composition is unlikely to be appropriate or sustainable,” the WHO Technical Advisory Group on Covid-19 Vaccine Composition (TAG-Co-VAC) said in a statement published on Tuesday.
2. Reported Infection Levels Among Vaccinated and Unvaccinated Citizens
Given that existing Covid vaccinations confer a form of immunity against infection that diminishes quite rapidly over time, in particular against Omicron, even in people who have already had two vaccinations, anyone who has not been very recently (say, within the past 4 or 5 months) double-vaccinated or boosted is likely to be at a risk comparable to that of the unvaccinated of getting infected and transmitting Covid-19.
So a very large proportion of citizens who would quality for a vaccination passport (under the new regulations now proposed for the EU, a Covid certificate would be valid for up to 9 months) would probably be transmitting the virus at comparable or potentially even higher rates to unvaccinated citizens (at least assuming that many unvaccinated citizens are already Covid-recovered and thus enjoy the superior immunity conferred by natural exposure to the virus).
Is this supposition borne out by official data on Covid infections? I believe it is, but I’ll let readers judge for themselves: to begin with, it is noteworthy that highly vaccinated countries like Israel, Denmark, Italy, Ireland, the UK, and Belgium (some of which have been operating vaccination pass systems until very recently), have seen Covid positive test rates (though thankfully, to a much lesser extent hospitalisations and deaths) go through the roof this winter. If Covid vaccines substantially reduced infection and transmission levels, it is hard to see how this could possibly happen.
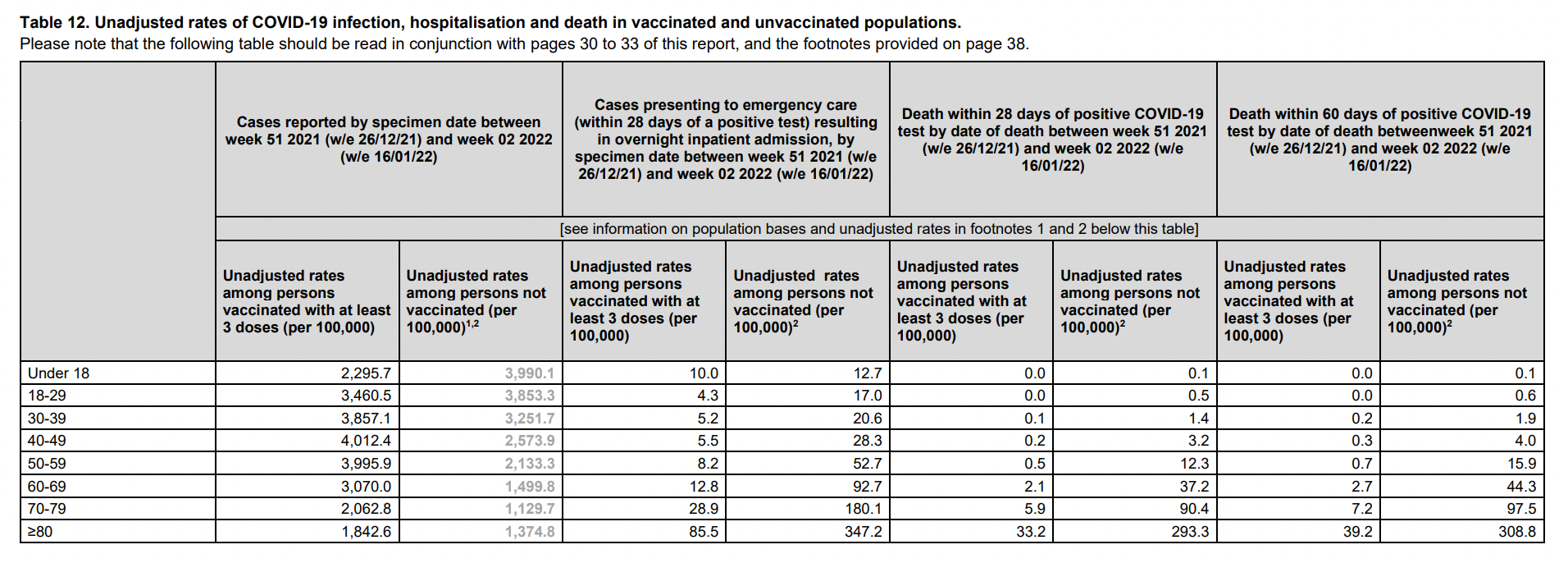
Now, let’s take a look at official test data collected by the UK Health Security Agency for week 3 of 2022. Embarrassingly enough for advocates of vaccine mandates, that data shows that the vaccinated population is testing positive for Covid-19 at similar levels from ages 18 to 39, and at nearly twice the rate as the unvaccinated population for ages 40 to 79.
Admittedly, these are not randomised tests and are subject to confounding factors. For example, if a disproportionate number of vaccinated citizens request Covid tests, this could artificially inflate Covid cases among the vaccinated. Nevertheless, even accounting for these possible confounding factors, this data casts serious doubt on the notion that vaccines provide substantial protection against infection or will significantly reduce community transmission of the virus.
Finally, let’s look at official test data drawn from 90,439 positive Covid cases occurring in Denmark in November and December 2021, analyzed by Denmark’s Statens Serum Institute, an infectious disease institute affiliated to the Danish Ministry for Health. Once again, we see a similar pattern: a disproportionately high number of positive Omicron-variant tests in the vaccinated population. Admittedly, the disproportion is not quite as dramatic as what we see in the UK data. But it is still quite striking. Within a national population that is 78% vaccinated:
- 89.7% of Omicron positive tests (out of 41,242 Omicron cases in total) analyzed in this sample occur in people who are fully vaccinated or double-vaccinated
- while only 8.5% of positive Omicron cases occur in the unvaccinated population
Once again, if vaccinated citizens present in larger numbers for tests, this could be a confounding variable. However, the fact remains that the overwhelming majority of Omicron infections picked up in this official Danish testing data occur in citizens who are vaccinated. This is very significant, given that Omicron is fast becoming the new dominant variant in many parts of Europe and the rest of the world.

With all of this data on the table, it is truly dumbfounding to me that any serious, scientifically competent public health authority could possibly believe for a moment that packing untested vaccinated people into bars and restaurants, or putting them on planes, and turning away their unvaccinated fellow citizens, will have a significant dampening effect on overall transmission dynamics for Covid-19.
What About “Nudging” People Into Making Better Health Choices?
If I am right, and vaccine passports are exceedingly unlikely to play any significant role in reducing Covid transmission, then there is only one remaining justification for their use: to penalise citizens for not making the best possible choices for their own health, and thus incentivise them to live healthier lives. One version of this argument values the citizen’s health independently of its wider social consequences; while another hopes to reduce health risks in the aggregate, and thus alleviate the burden on our health system.
The argument might go something like this:
- Even if vaccination is ineffective at reducing community transmission, there is evidence to suggest that vaccines may reduce the risk of hospitalisation and death, especially in older and sicker cohorts (these cohorts are disproportionately represented in Covid hospitalisation data).
- The inconvenience and cost of constant testing could induce an unvaccinated person into finally acquiescing and accepting a Covid vaccine, or getting that booster he had been holding out on for so long.
- We thus “save” that person from bad health outcomes.
- Furthermore, if we “convert” enough citizens to taking the vaccine – especially those in high risk categories – then we may reduce the aggregate burden on hospitals and healthcare providers.
This argument is not without its appeal, especially in a society saturated with a utilitarian narrative about public health. However, it is deeply problematic both from an ethical and medical standpoint.
From an ethical perspective, a vaccine passport scheme is basically a method for coercing people to undergo a specific medical intervention, thereby jettisoning the hallowed principle of informed consent to medical treatment. This principles exists to protect people’s reasonable autonomy from efforts by public or private actors to “manage” a patient’s health choices against their will.
Personal autonomy in the medical sphere is important not only for its own sake, but because it enables each patient to prudently weigh up all the relevant risks of a medical intervention in consultation with their doctor. Bulldozing over informed consent, even if it manages to reduce the collective disease burden (which is highly debateable, given the unintended harms caused by restricting patient choice, including poorly tailored risk assessments at the level of the individual patient, expert error, and reduced trust in public authority), will result in many individual harms, including medical tyranny, the imposition of medical risks unjustified by a patient’s personal medical history, and physical harms arising from medical interventions imposed under duress.
Furthermore, if we allow the use of vaccine passports as a strategy for pressuring citizens into making more responsible and enlightened health choices – whether for their own good or in order to take pressure off hospitals – then we should have no problem applying fines or penalties to smokers, excessive alcohol consumers, or the obese, since their behaviour is obviously elevating their own risks of hospitalisation, and taken as a collective, they are almost certainly increasing the burden experienced by hospitals and healthcare providers as well.
Those who accept the principle of medical coercion “for the patient’s own good” and/or for the sake of alleviating the burden on hospital capacity, should have no difficulty with turning the obese or smokers or excessive drinkers into second-class citizens until they “get with the programme” and mend their unenlightened ways. But many of us would balk at the prospect of a society that uses the coercive apparatus of the State to penalise and marginalise people until they agree to bring their lifestyles into line with “optimal” health outcomes, as defined by some remote body of “experts.”
Risks of Technocratic Calculations
An approach to public health of this sort would radically transform the relationship between rulers and citizens, by subordinating personal choice and prudence to the diktats of public health gurus who decide, based on the latest algorithms, which medications and lifestyles choices are most fitting to optimise citizens’ health. In this type of society, citizens would be subjected willy-nilly to technocratic calculations that can go badly wrong, in lots of different ways.
Here’s one way technocratic calculations can go badly wrong: population-wide directives, even if appropriate for a large number of citizens, may be very poorly adapted to some citizens’ personal circumstances and history. Consider the case of large-scale vaccination rollouts. Let’s assume that the Covid vaccines actually confer a clear benefit for large segments of the population. This does not necessarily mean that they confer a clear benefit on all cohorts of the population.
Consider, for instance, those citizens who are either young and healthy, or have gotten Covid-19 either once or twice already. For either of these groups, it is highly questionable whether the known and unknown risks of these novel vaccines are compensated by their medical benefits. We now know that the vast majority of Covid hospitalisations (according to this study published on the CDC website, 94.9%) involve patients with comorbidities; we also known that natural immunity is better and longer-lasting than vaccine-based immunity.2 So forcing the population at large, young and old, healthy and sick alike, to vaccinate is forcing many people to assume an unnecessary medical risk.
Another way technocratic calculations can go seriously wrong is that they may hubristically underestimate the risks of their systemic interventions. Consider once again the case of a large-scale vaccination rollout: by involuntarily subjecting an entire population to a relatively novel vaccine, rulers are coercively inflicting a giant medical experiment on everyone, with almost no exceptions. But neither the architects of these ambitious vaccination campaigns, nor anyone else, can guarantee that such an experiment will work out well for everyone, since nobody knows the long-term risks of these particular vaccines.
If people are free to opt out of such an experiment, then citizens can make their own risk assessments and the population-wide harms of the experiment will be limited by a self-selected “control group” that has chosen to opt out.
To sum up: there are two possible justifications for a vaccine pass system: first, that it will reduce Covid transmission. The evidence for waning immunity to infection in the months following vaccination, coupled with international data on infection levels among vaccinated and unvaccinated citizens, renders this justification completely implausible.
Second, one might argue that punishing the unvaccinated can pressure citizens to make choices more aligned to optimal health outcomes, whether at the individual or collective level. This justification fails because it assumes a highly paternalistic relation between political rulers and citizens, disregards the critical role of prudence in personal health choices, and underestimates the risk of technocratic, population-wide directives going badly wrong.
The sooner we bring an end to this embarrassing vax pass charade, the better for everyone.

