

On September 22 of last year, Michel Goldman, a Belgian immunologist and one of Europe’s best-known champions of medical research, walked into a clinic near his house, rolled up his sleeve, and had a booster shot delivered to his arm. He knew he’d need it more than most.
Just a few weeks earlier, Michel, 67, had been to see his younger brother, Serge, the head of nuclear medicine at the hospital of the Université Libre de Bruxelles, where both men are professors. Michel was having night sweats, and he could feel swollen lymph nodes in his neck, so his brother brought him in for a full-body CT scan. When the images came through to Serge’s computer they revealed a smattering of inky spots, bunched near Michel’s left armpit and running up along his neck. It was cancer of the immune system—lymphoma.
Given his own area of expertise, Michel understood this meant he’d soon be immunocompromised by chemotherapy. With another winter on the way—and perhaps another wave of SARS-CoV-2 infections—that meant he had just a narrow window of opportunity in which his body would respond in full to COVID vaccination. Having received two doses of Pfizer the prior spring, Michel quickly went to get his third. If he was about to spend months absorbing poison as he tried to beat a deadly cancer, at least he’d have the most protection possible from the pandemic.
Within a few days, though, Michel was somehow feeling even worse. His night sweats got much more intense, and he found himself—quite out of character—taking afternoon naps. Most worryingly, his lymph nodes were even more swollen than before. He conferred with Serge again, and they set up another body scan for September 30, six days before Michel was scheduled to start his cancer treatment. Once again he sat in the radiology waiting room while his brother waited for the pictures to appear on his computer.
Serge’s bushy eyebrows furrowed when he spoke with Michel after having seen the scans. (“I will always remember his face, it was just incredible,” Michel told me.) The pictures showed a brand-new barrage of cancer lesions—so many spots that it looked like someone had set off fireworks inside Michel’s body. More than that, the lesions were now prominent on both sides of the body, with new clusters blooming in Michel’s right armpit in particular, and along the right side of his neck.
When Michel’s hematologist saw the scan, she told him to report directly to the nearest hospital pharmacy. He’d have to start on steroid pills right away, she told him. Such a swift progression for lymphoma in just three weeks was highly unusual, and he could not risk waiting a single day longer.
As he followed these instructions, Michel felt a gnawing worry that his COVID booster shot had somehow made him sicker. His brother was harboring a similar concern. The asymmetrical cluster of cancerous nodes around Michel’s left armpit on the initial scan had already seemed “a bit disturbing,” as his brother said; especially given that Michel’s first two doses of vaccine had been delivered on that side. Now he’d had a booster shot in the other arm, and the cancer’s asymmetry was flipped.
The brothers knew this might be just an eerie coincidence. But they couldn’t shake the feeling that Michel had experienced what would be a very rare yet life-threatening side effect of COVID vaccination. For a doctor who had spent four decades studying and advocating for new medicines, that feeling would unfold into many months of deliberation and self-doubt. Michel used to run an institute for vaccine-technology research, and he’s spoken out to reassure the public about the safety of the COVID vaccines, and of the mRNA vaccines in particular. In December 2020, he told an interviewer that “if there was a real problem with the technology, we’d have seen it before now for sure.” His “main concern,” he continued, was that people would use the mere possibility of side effects “as an argument not to be vaccinated.”
But now that possibility appeared to be splattered all across his medical charts. Michel Goldman, champion of the mRNA vaccines, suspected that he was their unlucky victim.
Ihappened to speak with Michel by phone in April 2021, months before his cancer diagnosis. I’d called him to discuss another potential side effect of COVID vaccination, one associated in particular with the shot made by AstraZeneca. By that point, 220 people who’d received that vaccine had developed an unusual—and very dangerous—blood-clotting syndrome, which was characterized by an atypical low platelet count. At least seven people in the U.K. alone had died of the complication. Michel patiently laid out the different mechanisms that might explain this strange condition. But he was quick to add that the mRNA COVID vaccines were built in a way that could mitigate the risk of this particular problem.
Michel currently leads the I3h institute, a university hub aimed at assisting in drug-design projects; in an earlier posting, he headed a $2 billion European endeavor to accelerate the research of new medicines. As such, he’s spent many years attending to the possible risks—even tiny ones—of novel medical treatments. He has raised awareness about the iron overload that used to afflict dialysis patients before the advent of a drug known as erythropoietin, for example; and looked for signs of “cytokine storms” in kidney-transplant recipients who received monoclonal-antibody treatments. So when a plethora of new vaccines for COVID emerged in the first year of the pandemic, he was watching very closely.
When we talked about the potential side effects of the AstraZeneca vaccine last year, Michel made it clear that, in the big picture, any chance of serious complications from the shots would be orders of magnitude smaller than the chance of complications from the pandemic illness itself. If COVID vaccines caused clotting disorders or myocarditis in a tiny percentage of those who received them, he assured me, COVID would lead to stroke or heart inflammation in a much larger group.
The risks and benefits for each vaccine should be weighed against each other, he continued. If AstraZeneca were the only option, then its protection might be worth the very small risk of developing a rare blood disorder. But given the availability of Pfizer, Moderna, and other COVID vaccines, many people could opt for a safer alternative.
Now that risk-benefit calculation has been thrust upon him in a personal and terrifying way. By the time we spoke again, he’d become a cancer patient who suspected that his mRNA vaccine might have made things worse. Michel is reserved by nature, prone to making matter-of-fact remarks rather than emotive musings. In this case, I found him more guarded than ever, and I could tell he’d struggled over how he should describe his own experience—or, indeed, whether he should even be describing it at all. Perhaps his hypothesis was wrong, and the course of his cancer had had nothing to do with the shots. Or maybe the cancer and the mRNA vaccine were connected, but the risk of getting immunized was still just a tiny speck beside the benefits. Applying the same logic that he’d used before, he decided it made sense to go public with this theory. If other people with the same lymphoma felt the need to hedge their bets, they might consider holding off on the Pfizer and Moderna shots.
Michel knew that by speaking out about another potential rare effect—especially without hard proof—he’d be introducing a different kind of risk. Recent years had already seen a rise in anti-vaccine disinformation, and protesters have thrown menstrual blood at state legislators and issued death threats to public-health officials. Fearmongers have made the problem worse by citing scary-sounding data from the Vaccine Adverse Event Reporting System, a U.S. government database of possible side effects from immunizations, with insufficient context. In Europe, French police used tear gas to disperse anti-vaccine protesters who were aiming fireworks at officers in July of 2021; a vaccination center was set ablaze in Poland a few weeks later. Michel was well aware of all this trend; in fact, he’d been sounding the alarm about the spread of vaccine misinformation online before the pandemic even started. If he shared his own experience of cancer, might that make the problem worse?
This was not a reason to remain silent, Michel eventually decided. It was a reason to speak carefully.
First things first: Before Michel could tackle the conundrum of going public with this theory, he’d need to get his cancer under control. On October 6, he sat in a hospital room in Brussels, feeling quite afraid while nurses hooked up an infusion line to the catheter that had been surgically embedded near his collarbone. After so many years spent working as a doctor, he was suddenly a patient. People with his kind of lymphoma have only about a 30 percent chance of surviving longer than five years, and the aggressiveness of his disease meant that the medications would have to be intense. The drug that Michel was getting for his first infusion, called brentuximab vedotin, would be the newest and potentially riskiest in his regimen. Side effects can include breathing difficulties, blistering skin, and even permanent nerve damage.
Michel didn’t end up having any of those symptoms, but he did feel very weak. He convalesced at home, and for several days felt unable to do much of anything. But as soon as a bit of his strength came back, he started going through the cancer-research literature. He had several weeks until the next infusion, which meant he had several weeks to figure out whether the vaccine really had quickened his lymphoma, and whether other cancer patients might be in danger from the shots. He was used to reading stacks of science papers for his work; now he did so at an even faster pace.
Michel’s cancer was the kind that attacks the body’s T cells, which coordinate the immune response to invading pathogens. T-cell lymphomas come in roughly 30 different subtypes; Michel’s, known as angioimmunoblastic T-cell lymphoma, affects what are called follicular helper T cells, which hang out in the tonsils and the lymph nodes, among other tissues. Follicular helper T cells serve a crucial role in the cascade of events to protect the body after dangerous invaders have arrived. That process begins with dendritic cells, which identify a virus or other pathogen and present examples of it to the rest of the immune system. The helper T cells do just as their name suggests: They help pass that message along to B cells, which end up making protective antibodies against the virus.
Michel had recently learned that mRNA vaccines, such as the Pfizer shots he had received, are especially effective at generating that message, and spurring its passage through the helper T cells. Some researchers argue that the COVID vaccines from Pfizer and Moderna have been more protective than others for exactly this reason: They rev up those cells with extra oomph. Now Michel began to wonder whether that oomph could, in ultrarare cases, turn out to be a liability. Perhaps the shots gave such a jolt to his helper T cells that they went berserk. If they were prone to forming tumors, or if they were already cancerous, then overstimulation could have made the problem even worse.
As the days went by, Michel found other clues suggesting that the link was real, and that the mRNA vaccines might be risky for a specific subset of the population. He learned that body scans of some of those who get vaccines, including cancer patients, have shown heightened activity in the lymph nodes near the armpit on the side where the shot was received. He also came across another, very important clue. In 2018, a team of researchers based at Columbia University’s Institute for Cancer Genetics had published an intriguing study using mice with a pair of gene mutations that, when they co-occur, predispose T cells to go rogue. (Michel’s tumor, which had been sequenced by this point, showed the same two mutations.) When these mice were injected with sheep red-blood cells—as an experimental stand-in for invading microbes—the animals developed the subtype of lymphoma that was diagnosed in Michel.
Now Michel had a theory to explain the bleak coincidence that had befallen him. Serge agreed that it made sense. The brothers had co-written research papers in the past, including ones on the use of stem cells for heart repair and dendritic-cell vaccines for cancer. It was time for them to write another.
On october 20 of last year, Hans-Georg Eichler, a clinical pharmacologist and former senior medical officer for the European Medicines Agency, opened up his email to find a message from Michel. The two have known each other for more than a decade. “I hope that you are well,” the message started, “which is not really my case …” Michel had pasted in a link to a medical report, not yet published. “I am curious to hear your thoughts,” he wrote.
The paper, titled “Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot” and credited to Serge Goldman, Michel Goldman, and six of their Belgian colleagues, would run in the journal Frontiers in Medicine a few weeks later. (Michel is that journal’s editor in chief; he recused himself from the process of editing and peer review.) It begins by describing “a 66-year-old man with no significant medical history” who had been diagnosed with lymphoma that worsened following a booster dose of COVID-19 vaccine. The Goldmans’ unusual connection to the data—the fact that the 66-year-old man in question was Michel—comes across obliquely in the text. An ethics statement, printed at the end of the case report, includes the line: “Being one of the authors, the patient consented to the publication.”
Eichler, who had closely followed the furor over vaccine-associated blood-clot disorders the previous spring, replied that evening: “I have read the paper and am very impressed … It is the most responsible and courageous thing you could do under the worst possible circumstances.”
“I would say that 95 percent of the reactions were extremely friendly,” Michel told me later. But as he’d feared, anti-vaccine activists picked up on the story. “The lymph nodes of those who have taken these shots are exploding, burgeoning, and bulging with this toxic bioweapon,” a right-wing influencer named Jane Ruby wrote on Telegram beneath a screenshot of Michel’s CT scans, which had appeared in his published paper (and are reproduced in this article). “LYMPHOMA – That’s right… Cancer of the lymphatic system … STOP THIS FROM GETTING INTO BABIES AND CHILDREN!!!!!” Ruby’s claims were amplified on Natural News, among other anti-vaccination sites where, again, the very images that Michel’s brother had used to diagnose his illness were presented as shocking evidence of vaccination’s dangers. “PHOTOS: LYMPHOMA CANCER EXPLODING IN THE BOOSTED,” one website said.
When I told Michel about these online posts, he shook his head in disappointment. “They’re looking for anything to support their crazy vision,” he said. “It makes me sad about the world in which we are living.” That’s not to say he was surprised. Michel knew, for instance, that medical experts have dispelled false rumors about vaccines infecting people with COVID-19. He told me that he’d obsessed over getting the tone of the manuscript exactly right, so as not to fuel vaccine skepticism. He was careful, for example, to describe the vaccine as possibly “inducing” the “progression” of his cancer—rather than “causing” it to surface. “I spent hours and hours,” he said. “I’ve never spent so much time on details in a paper.” Extremely rare cases like Michel’s create a tricky terrain for science communication. Even a clinical trial with thousands of participants might never turn up a single case of someone’s cancer worsening after vaccination. In that context, experts can’t assign a statistical estimate of the risk across the wider population. Science journalists may be wary of reporting on the story for that reason. In fact, when Michel first told me about his cancer and about the paper he’d written with his brother, I said that I couldn’t write about it. I was worried that some readers would misinterpret my article, and mistakenly see it as a reason not to get vaccinated. As I write this, I’m still concerned that you might do exactly that. But the scientific literature is sprinkled with odd cases like Michel’s that have puzzled doctors. The Goldmans’ paper follows earlier isolated reports suggesting a possible link between COVID-19 vaccination and lymphoma. Aaron Mangold, who heads the division of clinical dermatology at the Mayo Clinic in Arizona, co-authored a paper published in May 2021 about a patient whose rare skin lymphoma recurred after his initial Pfizer shot. The tumorous ulcer appeared in the armpit of the same arm in which the man had received the injection, and then regressed spontaneously. A second shot of the vaccine, delivered three weeks later, produced no further lesions, Mangold told me, and the whole ordeal could have simply been a coincidence. He felt that he’d been “threading the needle” to go public with the case report given that uncertainty. Ladan Zand, a nephrologist at the Mayo Clinic in Rochester, Minnesota, faced the same conundrum when she co-authored a paper last year detailing five patients who had a relapse of kidney disease following mRNA COVID vaccination. Her team also documented eight patients who were newly diagnosed with the disease, known as glomerulonephritis, after receiving the shot. But Zand cautions that those patients might have had underlying kidney disease and not been aware of it. People infected with the novel coronavirus also show higher rates of kidney-function decline over time. “I spend half of my visits now asking patients to get vaccinated,” she said. “If you were to compare the risks and benefits, the benefits of the vaccine way outweigh the risk of rare entities that, for the most part, seem to be self-limiting.” William Murphy, an immunologist at UC Davis, told me that Michel’s before-and-after CT scans were fascinating in the context of the mouse study from Columbia. The cancer’s behavior certainly appeared to be related to the vaccine, he said, “given the huge difference in the scans of the tumor progression in a very short period of time.” But one can’t be certain, however striking the data. It’s just a case report, he added—one patient. The Goldmans’ paper, for its part, notes that it would be “premature” to extrapolate the findings from Michel to other patients with the same kind of cancer, and that the link, even if it were proved, should not discourage general uptake of “much-needed vaccines.” An unusual paragraph tacked onto the bottom of the article underscores the point. Marked “Patient Perspective,” and written in the third person, it notes that Michel himself “remains convinced that mRNA vaccines represent very efficient products with a favorable benefit-risk ratio,” and that he hopes the report will encourage further research. In mid-february, Michel spiked a sudden fever. COVID had finally caught up with him. Given that he was immunocompromised by six rounds of cancer chemotherapy, Michel knew that his doctors would need to act quickly. He soon received an infusion of the monoclonal-antibody drug sotrovimab, and managed to recover without incident; his lymph nodes stayed blessedly quiet, and there was no resurgence of his cancer. Now he’s eligible for a second booster shot, but he’s not sure whether he should take it. “I don’t know what I will do,” he said.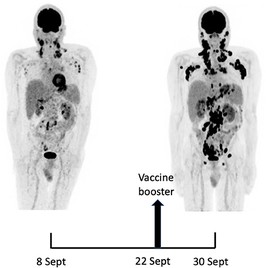
Would another dose of the vaccine cause another round of cancer lesions? Michel and the scientists who have been in touch with him are still mulling the evidence about whether his original cancer flare was simply a fluke. Steven Horwitz, a medical oncologist at Memorial Sloan Kettering who focuses on the care of patients with lymphoma, has looked more closely at vaccine side effects since hearing about Michel’s case, and feels reassured by what he’s found. “Of our patients who received mRNA COVID vaccines, we have not seen any clearly related and documented relapses or progressions,” he told me via email. Meanwhile, lymphomas and the treatments given for them can weaken the immune system, putting affected patients at higher risk of severe COVID-19 if infected. “Vaccination remains the most effective way to mitigate that risk,” he said.
I reached out to the makers of the mRNA COVID vaccines to ask about Michel’s case. A representative for Pfizer noted that the company takes such reports “very seriously” but that, “to date, there has been no identified correlation between the vaccine and cancer.” Moderna’s chief medical officer, Paul Burton, told me that the company keeps careful track of safety data and has not found any relationship between vaccination and lymphoma. He also pointed to the case of a 61-year-old woman with cancer of the salivary gland whose tumor shrank to about one-quarter of its original size in the month after she received a second dose of the Moderna vaccine. “Now, did it really regress because the person got a messenger RNA vaccine?” he asked. “I don’t know. I think biology is truly a remarkable thing.”
While Michel remains unsure about his fourth shot, he has continued to be outspoken on the benefits of vaccination overall, and often speaks to Belgian media on the topic. At the same time, he has become a stronger advocate for broader tracking of adverse events from vaccines—an endeavor he and others in drug development call “pharmacovigilance.” “We need to make sure that some pharmacovigilance programs are powered to detect very, very rare side effects,” Michel told me. Eichler, who was involved in drug regulation for the European Medicines Agency, said that while some doctors may be “aficionados” of randomized controlled trials as the only valid source of medical evidence, other types of information are needed. Michel’s case shows why: You’ve got a patient “who is a professor of medicine, who experiences the side effects and says, ‘Okay, this must be a side effect,’” Eichler said. That “rings the bells. Could Michel have ever come up in an RCT? My answer is probably not.”
Just a few days before Michel got COVID, he had gone back to Serge’s office for yet another set of full-body CT images, to check the status of his cancer. He sat in his brother’s waiting room, as he had last September, while Serge examined the results. This time, though, Serge’s expression was relaxed. The scans were clear.
Michel still has to watch out for a recurrence. And as a longtime immunologist and medical innovator, he’s still considering the question of whether a vaccine that is saving tens of millions of lives each year might have put his own in jeopardy. He remains adamant that COVID-19 vaccines are necessary and useful for the vast majority of people. But he wants the discussion about vaccines to be transparent.
Around the time of his February follow-up, Michel received a message from a doctor who had read his self-referential case report. The doctor’s mother had been diagnosed with the same subtype of lymphoma that Michel has following a COVID booster shot. More recently, he got an email from a woman whose sister had been vaccinated and received that diagnosis the following month. Again, these could be coincidences. Or maybe they are the second and third data points in a growing set. The possible connection between Michel’s lymphoma flare and his COVID-19 vaccination occupies much of his thinking these days. “If it exists, it must be very rare,” he said. But he doesn’t regret going public with his case. “I’m still convinced it was the right thing to do.”

